Irreversible electroporation
IRE– NanoKnife
“Problem solver” for lymph node and bone metastases – not only for prostate cancer
Lymph node, bone and organ metastases are present in many advanced-stage malignancies.
They represent tumor cell clusters of millions of cancer cells that have settled in the body outside the primary tumor and have their own blood supply by forming vessels and connecting to the patient’s vascular system.
How do metastases develop?

– Early detection
– Monitoring
– Detection of resistance mutations
Tumors, which themselves require a blood supply, are connected to the blood circulation of their “host”, the patient. Tumor cells, which are mobile, enter the bloodstream via the blood and lymph vessels. They can be detected there as circulating tumor cells (CTC – Circulating Tumour Cells) and by their genetic material. The detection method is called Liquid Biopsy.
Circulating tumor cells can attach to the inner wall of vessels and then actively migrate through the vessel wall. Outside the vessel, these tumor cells nest in connective tissues and can survive there from a few days to many years. These individual tumor cells, which are scattered throughout the body, have so far been diagnostically undetectable, even with the best imaging methods.
Provided that the individual tumor cell survives the attacks of the body’s own defense/immune system long enough, it can begin to proliferate in response to certain stimuli that are not yet fully understood. If the still small tumor cell cluster (micrometastasis) succeeds in forming vessels and connecting to the patient’s vascular system, it can grow into a metastasis, which can then also be detected by imaging (MRI, PET).

Why are metastases dangerous?
Like the primary tumor, metastases grow by proliferation of tumor cells. While normal cells stop dividing when surrounded by neighboring cells, tumor cells have lost this normal “social behavior” of cells. They continue to divide incessantly and destroy adjacent anatomical structures by pressure or by growing into them. Thus, metastases have the potential to destroy important endogenous structures (vessels, nerves, bones, etc.) and organs (liver, lungs, brain, etc.).
However, patients with tumor diseases often do not die as a result of such organ destruction, but from the sheer tumor mass. This is because tumor cells are recognized by the body’s own immune system as foreign to the body and are fought by the immune system. If the tumor mass becomes too large, the immune system exhausts itself fighting the tumor cells and the patients then often die from banal infections that the completely exhausted immune system can no longer control.
Tumor Mass Reduction
The key to longer survival in tumor diseases
If the tumor nodes growing in the body at different sites – so-called metastases – are identified by close-meshed imaging diagnostics (CT – computer tomography, MRI – magnetic resonance imaging, PET – positron emission tomography) and then selectively destroyed focally, these patients live longer ais patients in whom only systemic anti-hormonal or chemotherapy is administered in the case of an existing metastasis.
Focal destruction of metastases can occur in a variety of ways. The principle of tumor mass reduction is therefore an important key to longer survival of cancer patients.
Focal
Tumor mass reduction
with irreversible
electroporation ( IRE)
If imaging shows that only one or a few lymph node metastases are present, these can be destroyed – ablated – by inserting instruments into the lymph node through the skin (percutaneously), usually CT-guided.
At the VITUS Postata Center, we use an infrared guidance system (Cascination, Switzerland) for this purpose, which makes it possible to see the patient and his organs in virtual reality and to place the instruments needed for ablation in the metastasis with millimeter precision. This allows difficult approaches to metastases located deep in the body to be navigated without damaging vessels, nerves or organs.


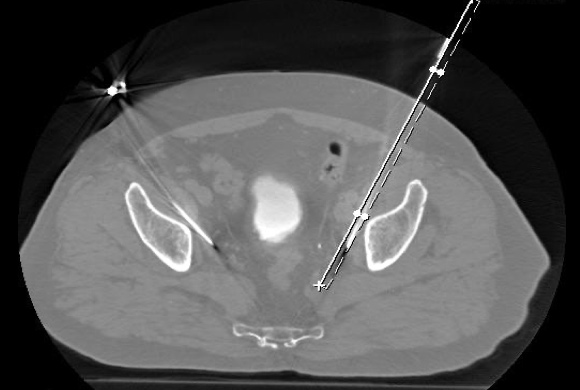
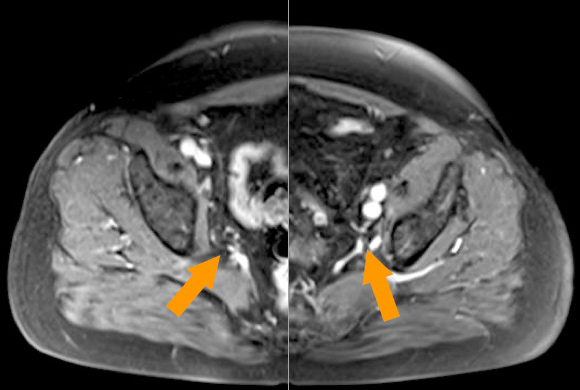
The images showed CT and MRI scans of a patient with lymph node metastases from prostate cancer. The patient had undergone hormone deprivation therapy (ADT androgen deprivation therapy) that was no longer working. The PSA level had risen to 8.65 ng/ml. The lymph node metastases (MRI image top right, arrows) are located deep in the pelvis in the area of the large iliac vessels (iliac vessels) and directly adjacent to the sciatic nerves (nervi ischiadici). The image on the top right shows the insertion of the electrodes into the lymph nodes in the computed tomography scanner using the infrared-guided virtual reality system Cascination. The CT image on the lower left shows the electrodes in their course from the abdominal wall to the metastatic lymph nodes. The MRI image on the right below shows the result five months later: the lymph node metastases have completely disappeared, and the PSA level dropped to 0.06 ng/ml.
Treatment of
bone metastases with
Electro-Chemotherapy
(ECT)
Minimally invasive and bone sparing
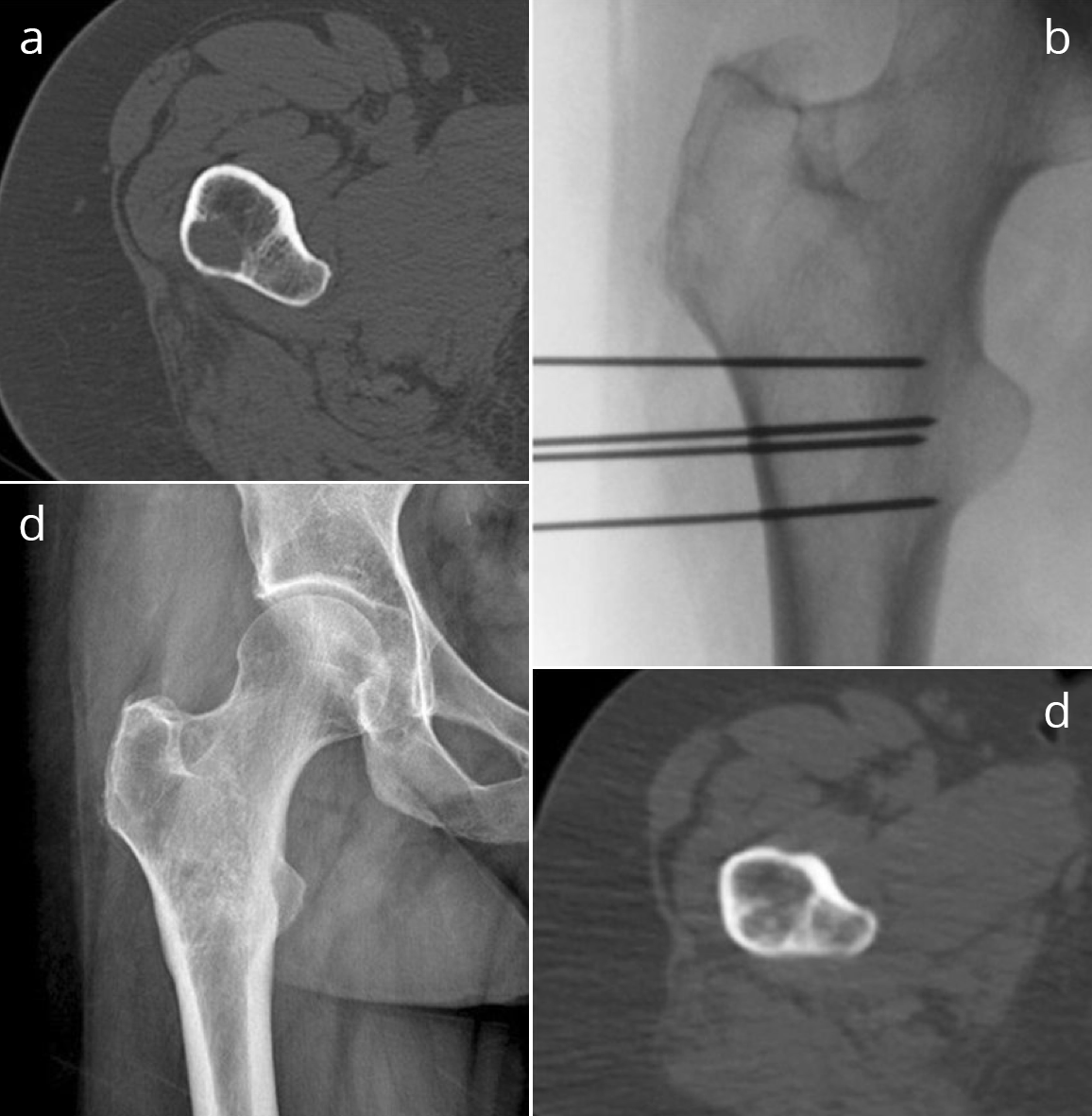
For bone metastases caused by prostate cancer, patients are usually treated with hormone deprivation therapy (ADT androgen deprivation therapy). However, this does not destroy the bone metastases, but only suppresses them, in most cases for 2 – 3 years. After that, the metastases continue to grow. Irradiation of bone matastases destroys not only the bone structure but also the blood-forming bone marrow and can lead to significant side effects such as a deficiency of red and white blood cells with an increased risk of infection.
Gentle treatment of bone metastasis is possible with the help of the so-called electro-chemotherapy. In this procedure, as in IRE, electrodes are inserted into the bone metastases. Instead of directly destroying the cells with current surges as in IRE, ECT uses gentler electrical pulses to create pores in the cell membranes. If the cell toxin bleomycin is administered at the same time, this preferentially penetrates the cells opened by electroporation and kills them. Cells outside the electroporation field take up the chemotherapeutic agent only poorly and are not or only slightly damaged. Little to no damage is done to the bone structure in this type of treatment for bone metastases. In particular, complete healing of the boil is possible after destruction of the metastasis(es), which is not the case with radiotherapy to the bone.
Other tumor mass reduction procedures
For lymph node, bone and organ metastases: Cyberknife
If insertion of the electrodes to destroy the metastases through the skin is not possible, irradiation with the CyberKnife can be used. This radio-surgical method makes it possible to reach metastases precisely even at sites in the body that cannot be reached percutaneously, e.g. because large vessels, nerves or intestines make safe access impossible.
In the case of extensive metastasis, where local tumor mass reduction is no longer possible, or in the case of complex structure of the metastases, e.g. in the pelvic bone, treatment with lutetium177 PSMA radiologand therapy can bring about systemic tumor mass reduction.
Let us advise you.
Make an appointment with one of our medical experts.
- Tumor mass reduction prolongs cancer survival time
- IRE and ECT allow destruction of metastases in lymph nodes, bones and organs without significant side effects on sensitive anatomical structures such as vessels, nerves and the bone structure
- Repeated use of tumor mass reduction, particularly for prostate cancer, can convert the primarily fatal cancer into a primarily chronic disease
- Effective tumor mass reduction can postpone hormone deprivation therapy (ADT, androgen deprivation therapy), since in most cases it is only effective for 2 – 3 years and is associated with massive side effects; ADT is thus available at a later time when, due to a too large number of metastases, effective tumor mass reduction is no longer possible with other means
- Repeated tumor mass reduction with IRE and ECT triggers secondary immune effects against cancer cells with each treatment, making the body’s defenses more effective in fighting cancer